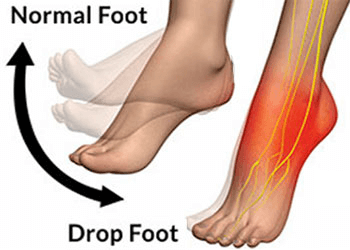
Foot drop is defined as weakness of tibialis anterior muscle on extending foot. It is caused by disruption to a nerve called the common peroneal nerve, usually due to LMN (lower motor neuron) disorder. This nerve controls primary ankle activity. Ankle joint, when it moves downwards, it leads to a lack of heel striking the floor during walking hence the term foot drop.
Source:
Foot drop is a clinical condition that is not commonly seen in primary care centres. Due to neurological shortcomings, there may be many aetiologies of foot drop.
Foot drop can go unnoticed. It is possible to have foot drop without being aware of the symptom. Individuals may walk as usual, but intermittently or repeatedly trip over themselves or feel like their footwear is loose. These symptoms may indicate an initial stage of foot drop due to nerve dysfunction and/or muscle weakness.
WHAT IS BEHIND FOOT DROP
1. Compressive Disorders:
Entrapment syndromes where a nerve is trapped between a tight muscle or a bony structure due to injury or a inter vertebral prolapse.
Compression or excessive pressure of a structure called the fibular nerve at some locations along the pathway it travels in body can lead to compressive neuropathy. This is the most common mononeuropathy affecting the leg and ankle.
The fibular nerve is present superficially near the head of the bone called fibula at the leg. This fibular nerve is vulnerable to pressure dysfunctions of nerves also known as pressure palsies. Sometimes you may have a condition of tight hamstrings muscle and a tight calf muscle. This can contribute to compression of the fibular nerve.
Other factors such as prolonged bedridden status, tight fracture casts, space-occupying lesions like cysts or tumors and cancer of the bone tissue involving the fibular head.
You may have compression of a structure called Sciatic nerve. This compression occurs between the two parts of a muscle in hip joint called the piriformis muscle thus leading to foot drop.
A condition called Lumbar radiculopathy (nerve pain and irritation) is considered as a common cause of foot drop. At the level of L5, radiculopathy is seen frequently and typically results from lumbar disc prolapse (herniation) or spondylitis in the spine.
A study done by Garcia Martinez MA et al, Compression palsies in the ICUs due to protracted bed rest have been observed. Approximately 10% of patients that stay in the ICU for a period longer than four weeks are expected to develop an altered sensation (paresis) of the fibular nerve. Critical illness, polyneuropathy, involving multiple nerves can also present with foot drop. Depending on the extent of involvement of the nerve, weakness can be in both the limbs (bilateral). Patients with diabetes are more vulnerable to these compression neuropathies.
2. Traumatic Injuries
Traumatic injuries such as muscle injury, knee dislocations, gun shot wounds, fractures, blunt trauma, musculoskeletal injuries etc.,
These injuries involve muscles, bones and nerves.
In clinics a common condition called Sciatic neuropathy, result from a traumatic injury of the hip or secondary to hip surgery.
Sciatic neuropathy is the second most frequently seen mononeuropathy of the lower limb and almost always presents with foot drop.
A rare cause of foot drop may be because of lumbosacral plexopathies (disorder of group of nerves), in this case you might have a traumatic injury to the back, a post operative complication of abdominal or pelvic surgery, or a complication of cancer cell growth or radiation therapy in already existing cancer.
3. Neurological Disorders:
ALS (Amyotrophic lateral sclerosis), also known as motor neuron disease (MND) or Lou Gehrig disease, an autoimmune disorder, is one of the reasons of foot drop. It is a neurodegenerative disease resulting from the death of important neurological structures (motor neurons) in the spinal cord and brain. This leads to muscle weakness, difficulty in speaking and swallowing. If you have ALS you may initially present with a painless foot drop.
Cerebrovascular disease (CVA) also known as Stroke, can present as hemiplegia extensive weakness and loss of sensation of one side of the body. Foot drop is a part of this presentation. If you have suffered from a stroke you may also have other signs such as increased muscle tone, overactive responses of muscles, and circular movement of hip joint of the lower extremity during an attempt to walk. Depending on the location of blood supply cut, absence of speech can also be present.
Acute inflammatory demyelinating polyneuropathy (AIDP), also known as Guillain-Barré syndrome, is an autoimmune disorder. A process in which there is progressive motor (muscle) weakness, sensory loss, and loss of reflexes are the prime characteristics. Foot drop can be imminent in this whole disorder. Sensory loss often comes before muscle (motor) weakness. There is a damage to the protective covering which encapsulates the nerves to brain and nerve structures (myelin sheath) and this leads to segmental damage to the covering of nerve fibres called as demyelination. A typical sign of Guillain-Barré is the slowing of nerve conduction velocities and conduction block when monitored under NCV machine.
Poisoning Of Dangerous Substances: Toxin induced neuropathy is another common reason for foot drop. Some are listed below.
Lead Poisoning.
Elemental Mercury poisoning.
Organophosphate poisoning.
Arsenic poisoning.
Alcohol poisoning.
Drug overdose.
Epidemiology Of Foot Drop in India
In 2012 Dhillon MS, Aggarwal S, Dhatt S, Jain M did research on Epidemiological Pattern of Foot Injuries in India: Preliminary Assessment of Data from a Tertiary Hospital. They found that about 7.4 percentage of 1765 patient population that came for treatment had foot drop.
HOW DO THE DOCTORS MAKE A DIAGNOSIS:
A team of neurologist experts do the following examination which leads to appropriate diagnosis.
1. Careful neurological physical examination.
2. A metabolic blood work-up to rule out diabetes.
3. Electromyography /Nerve Conduction Study.
4. MRI /CT scan (imaging).

Source: hopkinsmedicine.org
It imperative that you do not self diagnose because adequate knowledge of anatomy and physiology is essential to arrive at the appropriate working diagnosis, as the management will depend upon a correct diagnosis.
A thorough examination by the physiotherapist is intended to review the evaluation of the neurologist and to understand the root cause behind foot drop (pathophysiology). As in the management of foot drop, physiotherapy techniques vary from condition to condition. There is an important role of the interprofessional team in evaluation, management, and potential treatment of patients presenting with a finding of foot drop.
Treatment:
1. Treatment for foot drop includes several Physiotherapy techniques and/or splinting and medication given by healthcare provider to manage your pain.
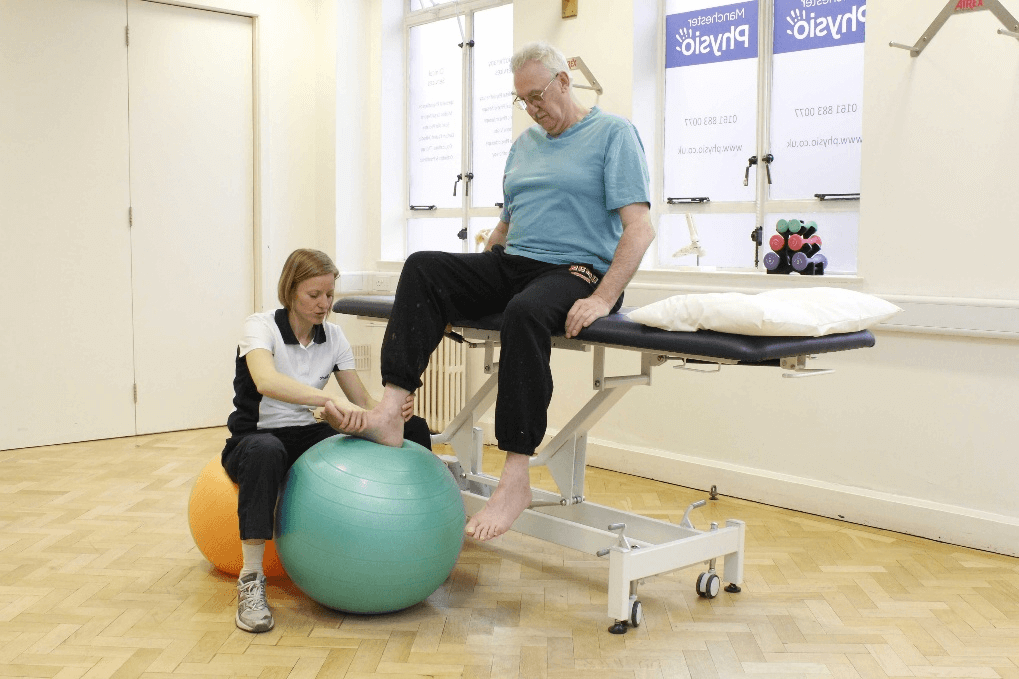
2. The goals of Physiotherapy management are to stabilize the walking pattern, prevention of contracture formation, maintain the muscle activity and to prevent falls. Physiotherapy management focuses on stretching and strengthening the foot muscles.
Source: medicalnewstoday.com
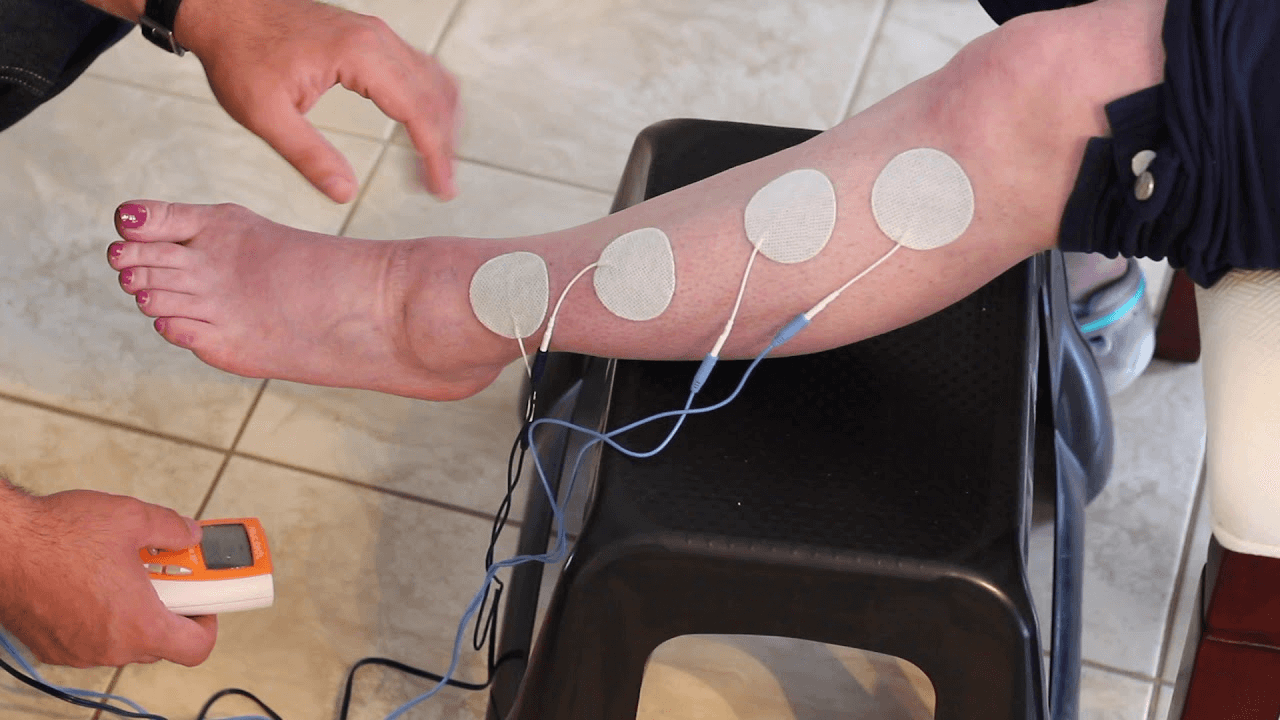
3. Electrical stimulation techniques with EMT machine of the weak foot muscles have shown great results. Functional electrical stimulation works wonders.
Source: researchgate.net
4. A gentle exercise program will be an important part of Physiotherapy- specifically to maintain the muscle activity, strength and range of motion of muscle groups that are working in the prevention of flexion contracture.
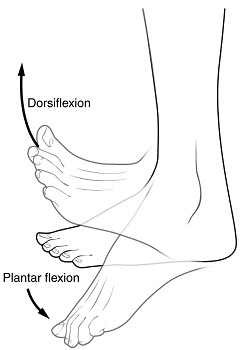
5. Splinting (securing the ankle joint with a crepe bandage or splint) is used to minimize contractures. For complete nerve damage with insufficient recovery, an ankle-foot orthosis (AFO) to prevent further foot in bent position (plantarflexion) is advised.

Source: tynor.com
Source: physio.co.uk
6. Physiotherapist provides sufficient education to the patient and training to handle the condition. It is imperative to learn in the proper usage and maintenance of the brace.

Source: flintrehab.com
7. If you have foot drop with numbness, your Physiotherapist will give you a sensory box to maintain the sensation to the affected part. Also, the instructions for skincare to prevent cuts, abrasions and ulcer formations are given as they will prove significant in recovery.

Source: sensorykit.com
8. You will also receive instructions from an orthotist as part of management and the help is often found useful if you have any problems with your AFO. It will be coordinated with your orthotist to modify the orthosis while fabricating the AFO.
9. For pain management your health care provider will prescribe topical analgesics to be applied over painful area. But these medications are temporary just to relieve pain and will not likely result in clinical recovery.
10. You will be asked to follow up electrodiagnostic studies to monitor the progress and reassess the situation, as watching out for reinnervation of the foot is an important part of the treatment planning.
Reference:
Subhadra L. Nori; Michael F. Stretanski. Foot Drop. Treasure Island (FL): StatPearls Publishing; 2021 Jan
García-Martínez MÁ, Montejo González JC, García-de-Lorenzo Y Mateos A, Teijeira S. Muscle weakness: Understanding the principles of myopathy and neuropathy in the critically ill patient and the management options. Clin Nutr. 2020 May;39(5):1331-1344.
Carolus AE, Becker M, Cuny J, Smektala R, Schmieder K, Brenke C. The Interdisciplinary Management of Foot Drop. Dtsch Arztebl Int. 2019 May 17;116(20):347-354
van Zantvoort A, Setz M, Hoogeveen A, van Eerten P, Scheltinga M. Chronic lower leg pain: entrapment of common peroneal nerve or tibial nerve. Unfallchirurg. 2020 Jan;123(Suppl 1):20-24.
Greenberg M. Handbook of Neurosurgery. New York, NY: Thieme Medical Publishers; 2001.
Burridge JH, Taylor PN, Hagan SA, Wood DE, Swain ID. The effects of common peroneal stimulation on the effort and speed of walking: a randomized controlled trial with chronic hemiplegic patients. Clin Rehabil. 1997;11:201–210.
Pisciotta C, Shy ME. Neuropathy. Handb Clin Neurol. 2018;148:653-665.
Punjani R, Wagner L, Horton K, Kaye W. Atlanta metropolitan area amyotrophic lateral sclerosis (ALS) surveillance: incidence and prevalence 2009-2011 and survival characteristics through 2015. Amyotroph Lateral Scler Frontotemporal Degener. 2020 Feb;21(1-2):123-130.
Leung J, Sejvar JJ, Soares J, Lanzieri TM. Guillain-Barré syndrome and antecedent cytomegalovirus infection, USA 2009-2015. Neurol Sci. 2020 Apr;41(4):885-891.
https://www.researchgate.net/publication/269661361_Epidemiological_Pattern_of_Foot_Injuries_in_India_Preliminary_Assessment_of_Data_from_a_Tertiary_Hospital